As an industry we love to throw out numbers, the most repetitive being 500 mL. We hear that number several times over the course of our initial training courses. And I do not know about the other DistanceCME (DCME) faculty, but I feel like I mention 500 mL at least once a week, and usually more. As an industry, is the emergency medical services (EMS) industry a fan of numbers? Generally, the answer is no. And if you start emailing me talking about how you love math, I am going to make a motion in our monthly EMS union meetings to have you voted off the island.
Fluid Loss
So, what is 500 mL in the real world? A16.9-ounce bottle of water is exactly 500 mL. A lot of us carry these bottles with us on duty and in our daily lives. Some of course carry around a soda bottle, which is also the same measurements. Over the course of a 24-hour period our bodies produce 16.9-ounces of cerebral spinal fluid. Normal blood loss after a vaginal childbirth is 16.9 ounces, which should be collected in a Chux pad so that it can be weighed in labor and delivery to ensure mom has not lost too much blood.
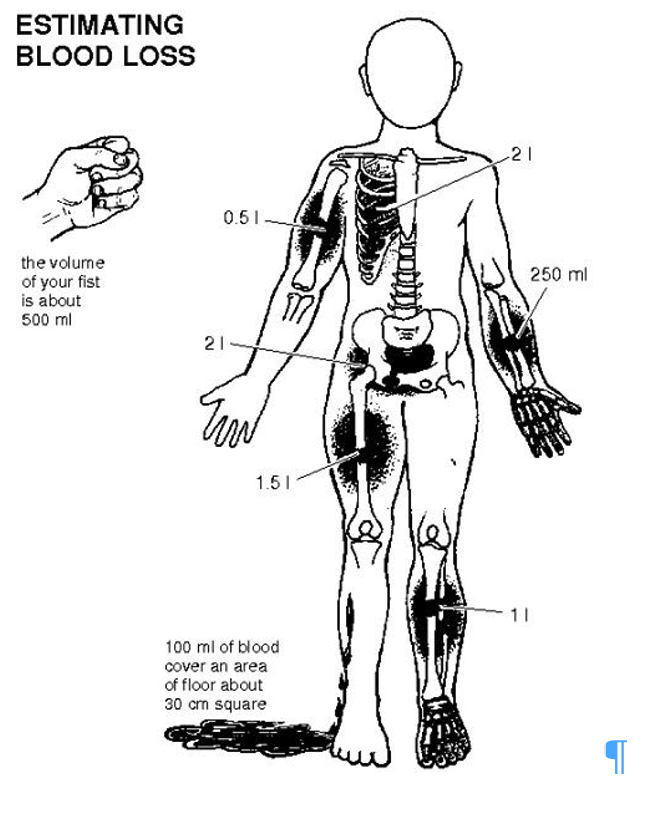
Estimating blood loss is very challenging. If you take a 16.9-ounce (500 mL) bottle of water and pour it out on the ground, what happens? As it spreads out across the ground it looks like there is a lot more volume than there really is. It looks like a crime scene. We do know when people injure specific areas of the body, there is a maximum amount of blood loss that can occur, if the fracture is a closed fracture.
- Radius/Ulna – 250 – 500 mL (1/2 – 1 16.9-ounce water bottle)
- Humerus – 500 – 750 mL (1 – 1 ½ 16.9-ounce water bottle)
- Tibia/fibula – 500 – 1,000 mL (1 – 2 16.9-ounce water bottles)
- Femur – 1 – 1.5 L (2 – 3 16.9-ounce water bottles)
- Pelvis – 2 L, 4 L if the patient is pregnant and in the final weeks of pregnancy. (4 – 8 16.9-ounce water bottles
Tidal Volume
And then we have adult tidal volume (500 mL) – dead space (150 mL) = 350 mL, which is approximately 1 12-ounce soda can, or you can substitute for whatever your favorite canned beverage might be. And when you think about it in these terms can you see why shortness of breath is the most subjective complaint a patient can have? We only have on soda can participating in gas exchange. It does not take much to create a ventilation/perfusion mismatch. So even though you cannot see the external signs of difficulty breathing the patient is struggling. They just called you early, which is what we want them to do. And if you do not take their complaint seriously, are they going to call 911 early in the future? Probably not.
Another number connection we can make is ventilations. How often do ventilate a child or infant? Thankfully, not very often. But we ventilate adults with an advanced airway in place on a regular basis and we know it’s a ratio of 1:6 seconds. When we must take care of a child, we simply divide the 6 in half, 1:3 seconds. And then for a newborn/infant, divide the 3 in half and our rate is 1:1.5 seconds. And another rare instance is a patient that is presenting with signs of brain herniation. The hyperventilation rate for an adult head injury patient is the same ventilatory rate as a child, again divide the 6 by 2 and we have an adult hyperventilation rate of 1:3.