Airway management is often a skill that Paramedics and Critical Care Paramedics are thought to be experts on. It is a skill that we often practice, practice again and then practice again to become comfortable with. One pitfall of being an advanced provider is the fact that many advanced providers look for the shiny object in the room rather than focusing on the more basic, less glamorous interventions. Basic level providers often are the playing field leveler for the airway management process. They do this by grounding the advanced provider and reminding them that not EVERY airway needs and endotracheal tube to be managed. I have often said that i would much rather work with a good, practical EMT than an arrogant, overconfident paramedic and to this day, I stand by statement. Today we are going to discuss airway management techniques and effective practices in managing a patient’s upper airway.
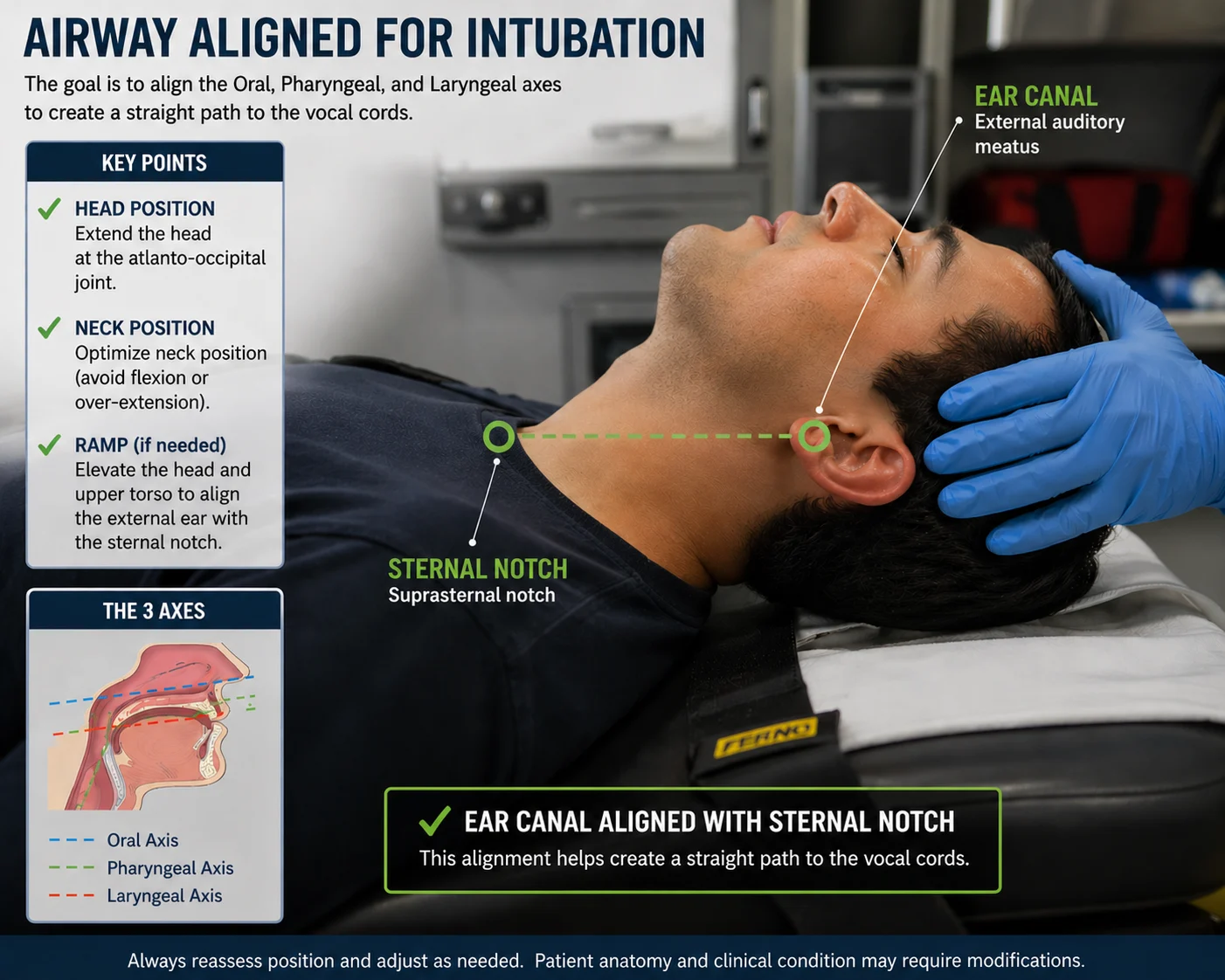
Anatomically, the upper airway is everything above the level of the glottic opening or vocal cords. The upper airway is the conduit of the respiratory system. It allows the inhaled gasses to travel down past the glottic opening in hopes of achieving gas exchange at the alveolar level, which is part of the lower airway. The main goal of managing the upper airway is establishing and maintaining patency. Proper positioning is crucial in order to maintain a patent, effective airway. Proper positioning is often overlooked by advanced providers that look directly towards the end goal of endotracheal intubation. Proper positioning varies based on the age of the patient. Newborns, neonates and infants often have a very large occiput area on the back of the skull. When placed supine on a flat surface, this large occiput can cause the chin of the small patient to migrate towards the sternum, thus partially or completely occluding the airway. Padding under the shoulders or torso of the young pediatric patient accommodates for the large posterior occiput and therefore helps to maintain a patent, neutrally positioned airway. Hyperextension should also be avoided in the younger pediatric patients because their airway is much smaller in diameter, more flexible and positioned slightly more anterior. Hyperextension of the head can actually work against maintaining a patent airway in this population and studies have shown that a neutrally positioned airway tends to be more patent than a hyperextended airway in this age group. Older pediatric patients and adults have a larger diameter airway and are less likely to experience airway collapse due to hyperextension. In the older pediatric population and adult population, we often will place padding behind or under the occiput of the head. This puts our patient in the “Sniffing Position”. Our upper airway has three axis: the oral axis, the pharyngeal axis and the tracheal axis. The oral axis is virtually perpendicular to the floor when our patient is in the supine position. The tracheal axis is virtually parallel with the floor when our patient is in the supine position. The pharyngeal axis runs at about a 30-40 degree angle to the floor when our patient is in the supine position. Whether we place padding under the torso or shoulders on the young pediatric patient or under the occiput on the older pediatric or adult patient, our goal is to align these three axis of the airway.
We were all taught the head tilt-chin lift maneuver or the modified jaw thrust maneuver in CPR class and during our initial education. This maneuver only aligns 2 of the 3 axis: the oral and the tracheal axis. Think about this for a moment. When was the last time you saw a conscious patient in respiratory distress, just throwing their head back and hyperextending their neck? More often they tripod if possible, and then place their airway in the “sniffing position”. This is not something that is learned. This is an instinctual attempt to align the three airway axis to minimize obstructions and maximize air flow. In order to most effectively align the 3 away axis in our supine patients, we must add padding to our positioning attempt. As we said earlier, padding under the shoulders/torso for the young pediatric patient and padding under the occiput for the older pediatric or adult patient. Aligning the 3 axis of the airway promotes that optimal airway positioning and often improves upper airway patency by limiting obstructions. A good rule of thumb is to align the opening of the ear on a parallel plane with the sternal notch. Keep in mind, that we always want to be cognizant of potential cervical spine injuries but we must prioritize treatment modalities. Which would you rather have: a live patient that MAY have a cervical spine injury or an intact, uninjured cervical spine on a morgue table? In addition, studies have shown very little risk of cervical spine injury worsening with gentle c-spine manipulation which may be needed to establish that patent, maintainable upper airway.
Remember, always try to work smarter, not harder. Many healthcare and more often EMS interventions are based on anecdotal evidence that is not supported by data. Legacy interventions like just the head tilt-chin lift or the modified jaw thrust maneuvers were the best we had “Back In The Day”. But we know better now. Large data collection and proper analysis have proven the effectiveness and safety of the sniffing position in our patients that require proper airway alignment. Always remember that we shouldn’t just do something because someone told us or taught us to do it that way. Lets base our patient care interventions on the most up to date information at our disposal.